Case study: Seaplane medical evacuations in South Florida

A 79-year-old man experienced a cardiac arrest while on a cruise ship in the Caribbean and was medevaced by seaplane back to the USA. Steve Williams, Senior Director, Global Air Medical Operations, REVA Air Ambulance, describes the case
REVA Air Ambulance operates 16 aircraft from four bases in Fort Lauderdale, Florida; San Juan, Puerto Rico; Schenectady, New York; and Shannon, Republic of Ireland. Several of our cruise line clients schedule their cruise ships to dock at small private islands in The Bahamas. Most of these small private islands do not have easy access to traditional fixed-wing air ambulance operations due to the lack of an accessible airport.
In partnership with Tropic Ocean Airways based at Fort Lauderdale Airport, REVA now provide medical evacuation flights utilizing float-equipped Cessna Caravans. The conversion of a regular float plane to an aquatic air ambulance able to provide intensive care unit (ICU)-level care was led by Sean Bryan, Director of Medical Operations, Western Hemisphere at REVA. This aircraft provides a cost-effective evacuation option from these small islands for cruise line guests or crewmembers who require urgent hospital admission.
Case presentation
On 18 March 2023 at 14:05 hrs, the REVA operations center received a call from a cruise line client that had a 79-year-old male US citizen who had experienced a ventricular fibrillation cardiac arrest. At 13:00 hrs, the patient was sitting on the balcony outside his cabin when his wife found him unresponsive. The shipboard medical team immediately responded and were able to resuscitate the patient and establish return of spontaneous circulation (ROSC). The patient was defibrillated four times during the resuscitation. The patient was transferred from his cabin to the medical center on the ship where the patient was intubated with an endotracheal tube and mechanical ventilation was initiated.
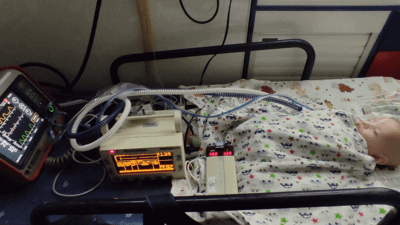
Our air medical team of three critical care flight nurses launched from Fort Lauderdale Airport in a seaplane and arrived at the small Bahamian Island at 17:30 hrs. We found the patient on the beach in the care of the ship’s medical team on the back of a small ‘Gator’ four-wheel drive golf cart just adjacent to the Jet Ski dock where we had tied up the seaplane.
After a rapid, focused clinical report, we assumed care of the patient and switched him over to our transport ventilator, moved his intravenous medications to our infusion pumps and then loaded the patient and his wife into the seaplane
After a rapid, focused clinical report, we assumed care of the patient and switched him over to our transport ventilator, moved his intravenous medications to our infusion pumps and then loaded the patient and his wife into the seaplane. Vital signs on handover were a blood pressure of 129/82mmHg, a heart rate of 97bpm with regular sinus rhythm, and with blood pressure being supported by dobutamine at 7µg/kg/min. The patient was being mechanically ventilated in Assist-Control mode at a rate of 14 breaths per minute, tidal volume of 400cc, with a fraction of inspired oxygen (FiO2) of 100%, and +5cmH2O positive end-expiratory pressure (PEEP). On these settings, the patient had an oxygen (O2) saturation of 100%, so the FiO2 was reduced to 90% with an O2 saturation ranging between 97–99% for the duration of the transport. Endotracheal tube placement and the security of the tube were checked prior to moving the patient to the aircraft. Sedation was maintained with Diprivan (propofol) and midazolam, with one additional bolus dose of rocuronium given during flight to maintain paralysis. During the 45-minute flight back to Fort Lauderdale, the cardiac monitor showed increasing ventricular ectopy characterized by increasing rate of multifocal premature ventricular complexes (PVCs) and so the patient received a third intravenous bolus of amiodarone (150mg), and an amiodarone infusion was commenced at 1mg/min. The patient’s cardiac rhythm then settled with fewer episodes of multifocal PVCs.

After the aircraft landed at Fort Lauderdale Airport, the patient was transferred to a ground ambulance and taken to the local hospital. The patient was taken for immediate cardiac catheterization, which did not demonstrate any significant coronary artery lesions. The patient had an automatic implantable cardioverter defibrillator implanted and was discharged from the hospital after five days to a rehabilitation unit, and finally returned home to continue his recovery on 4 April 2023. Follow-up with the patient was conducted after nine months; the patient was happy and healthy, and has returned to his pre-cardiac arrest activity without any neurological deficits, including continuing to sail on cruise ships.
A retrospective study in 2016 of 67 cases of cardiac arrest on one large cruise line demonstrated a rate of ROSC or successful resuscitation of 30%
Discussion
Over the last 15 years, the cruise industry has really improved the quality of medical care available onboard. A retrospective study in 2016 of 67 cases of cardiac arrest on one large cruise line demonstrated a rate of ROSC or successful resuscitation of 30%, which is a great credit to the professionalism and training of cruise line medical personnel. This patient certainly owes his life to the rapid response of the cruise line medical staff in this case.
May 2024
Issue
In our special training edition for May, find out how operators of all sizes are using new tools and equipment to train their pilots; discover what is the latest in technology for training hoist and winch operators; learn how air medical crew remain current and up to date with the latest techniques and procedures; and find out what goes into the essential medical kit bags that are carried into the skies; plus more of our regular content.
Steve Williams RN
Steve Williams is the Senior Director, Global Air Medical Operations, with REVA. Steve qualified as a registered nurse in London in 1986 and started work as a flight nurse in 1990. Prior to working at REVA Steve also spent 17 years as Director Fleet Medical Operations at Carnival, Royal Caribbean and MSC Cruises. Steve also serves as Deputy Team Commander for the US Government’s Trauma and Critical Care Team, deploying on multiple missions as a disaster medical response specialist.